GLP-1 Peptides: Weighing the Risks, Benefits, Costs, and Ethical Implications
by Dr. Mark Cucuzzella and Dr. Andrew Koutnik
Mark Cucuzzella, MD, FAAFP is a physician at Houlton Regional Hospital in Maine and member of the Coalition for Metabolic Health’s Scientific and Clinical Advisory Committee.
Andrew Koutnik, PhD, is a principal investigator and research faculty at Florida State University’s Institute of Sports Sciences and Medicine, a visiting research scientist at the Florida Institute for Human and Machine Cognition, and a member of the Coalition for Metabolic Health’s Scientific and Clinical Advisory Committee.
“Assess the prevalence of and threat posed by the prescription of…weight-loss drugs”
GLP-1 receptor agonists and dual GLP-1–GIP receptor agonists (hereafter referred to as “GLP1s”) have been described as a revolution in obesity and type 2 diabetes management. These peptides, including semaglutide and tirzepatide, mimic elevated GLP1 to supraphysiologic levels to regulate blood sugar levels and appetite. However, like any medical intervention, there are limitations and risks.
As the nation tackles the obesity epidemic now affecting over a 1/3 of the U.S. population and its widespread impact— including the high cost of public prevention, the unsustainable expense of medical treatment, and the physical and economic burden of the disease— we must explore effective and cost-effective therapies and treatment optimization.
The unfortunate “necessity” of these medications is discussed in other sections of this report. In public health, we all recognize that prevention is more effective than treatment. Unfortunately, a significant portion of the population requires intensive intervention. Many patients with obesity and/or prediabetes go undiagnosed and untreated leading to disease progression. GLP1 use will continue to grow as their approved indications expand, drugs become more effective, and ideally, costs will eventually align with global standards. However, risks and limitations have emerged.
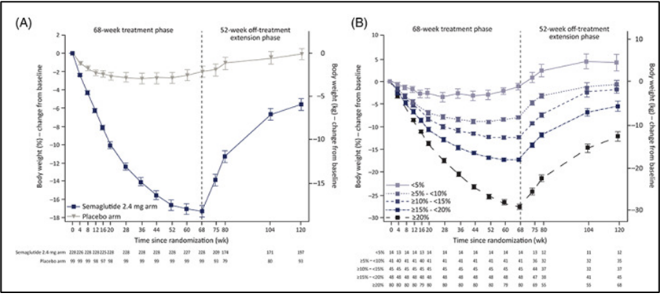
Pharmaceutical and medical claim records indicate that 68% of patients discontinue GLP1 drug classes within 1 year of initiating. Most notably, upon medication cessation, weight regain is rapid leading many public health officials to argue that patients must remain on them indefinitely marking an unsustainable public health dilemma.
Drug cost can often exceed >$12,000/year with analyses from the Institute for Clinical Economics Review demonstrating that GLP1 drugs cost two-fold higher than their expected value from weight-loss-associated reductions in cardiovascular events and diabetes lifestyle management. Historically, major supplies (Eli Lilly and Novo Nordisk) cannot match healthcare demands, limiting access. 30-50% of people with diabetes report anxiety and/or fear of injections, which may be even higher in the general public who are unfamiliar with continuous syringe or needle treatments. There are also several known acute and chronic side effects of GLP1a administration.
Potential Risks (not all-inclusive):
- Common gastrointestinal side effects: nausea, vomiting, diarrhea (30-50% of users) [1] [2]
- Potential loss of lean mass (25-40%) [3
- Rare but serious risk of acute pancreatitis [4] [5]
- Increased risk of gallbladder disease, including gallstones [6]
- Potential for acute kidney injury, especially due to dehydration from GI side effects [7] [8]
- Possible increased risk of thyroid cancer (though human data remain inconclusive) [9]
- Risk of hypoglycemia when combined with insulin or sulfonylureas [10]
- High cost and discontinuation rate [11]
However, as GLP1 only works so long as they are continually administered, some speculate that life-long administration may be required and the long-term effect of these drugs beyond 5 years remains largely unknown. While inherent limitations are revolving these limitations require alternative cost-effective lifestyle treatments, this document provides a fundamental overview of the benefits, risks, and costs of the medication. More importantly, it offers a framework for clinicians to assess appropriate use and optimize treatment. Our discussion will be guided by the Four Pillars of Medical Ethics, which safeguard patients from harm while enabling physicians to follow their conscience and exercise professional judgment. Any conversation about these medications must be intertwined with the principles of medical ethics.
1st Pillar of Medical Ethics: Autonomy
Patient self-determination is a fundamental principle in medical treatment, encompassing informed consent, confidentiality, truth-telling, and protection against coercion. Genuine informed consent is an ongoing process that requires a competent patient, full disclosure of the proposed treatment, clear understanding, and voluntary agreement. When it comes to GLP1s, true informed consent must include a thorough discussion of its potential benefits, known and unknown risks, and the necessary support and behavior changes for optimal use. Only through this approach can we ensure the effective medical and financial use of this medication on a national scale. Over the past decade, countless articles have explored the growing list of medical indications and potential benefits of these highly sought-after medications, alongside their associated risks [12] [13] [14] [15] [16] [17] [18] [19] [20] [21].
2nd Pillar of Medical Ethics: Beneficence
The second pillar of medical ethics, Beneficence, requires physicians to act in the best interests of their patients. Every treatment or procedure should provide a clear benefit to the individual receiving it. If a procedure offers no advantage to a patient, it should not be performed. Ethical medical practice prioritizes personal well-being over collective interests.
GLP1 Potential Benefits (not all inclusive):
- Significant weight loss (10-20% in obese patients at over a year) [22] [23] [24]
- Improved glycemic control in type 2 diabetes [25] [26]
- Reduced risk of major adverse cardiovascular events [27] [28]
- Improved kidney function and slowed progression of diabetic kidney disease [29] [30]
- Potential neuroprotective effects for conditions like Alzheimer’s and Parkinson’s [31] [32]
- Reduced addiction to substances like alcohol and substance use [33] [34] [35]
- Reduced visceral fat and liver fat [36] [37]
- Improved musculoskeletal health [38] [39]
It is also essential to lay out alternative treatment paths. Most notably, low or no-cost nutritional intervention.
Low-carbohydrate or ketogenic diet benefits (not all inclusive):
- * Significant weight loss (10-20% over a year)
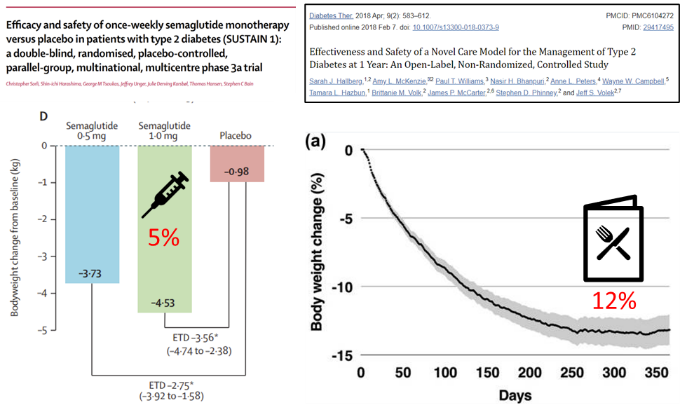
- Weight loss is greater with low-carbohydrate and ketogenic diets (10-15%) in type 2 diabetes than current GLP1 (5%) [40] [41]
- Type 2 diabetes remission in >50% of patient (<5.7% HbA1c without medication) [42] [43] [44]
- Reduced metabolic-associated steatotic liver disease (previously known as Non-Alcoholic Fatty Liver Disease).[45] [46]
- Deprescription and annualized healthcare cost savings $5000/patient to >$10,000/patient.
- Demonstrated ability to off-ramp GLP1a [47] [48]
- Juvenile diabetes (<5.7% HbA1c with only medicinal insulin) [49] [50] [51]
- Rapid reversal of prediabetes (<4 weeks) [52] [53]
- Seizure reduction in drug-resistance epilepsy [54] (~10% of patients with epilepsy are cured after diet cessation [55])
- Improved cognition and mental state in Alzheimer’s [56] and age-related cognitive decline [57]
- Potential ability to improve kidney disease [58]
3rd Pillar of Medical Ethics – Non-Maleficence
The third pillar of medical ethics, Non-Maleficence, is rooted in the principle primum non nocere—“First, do no harm.” Any treatment or procedure with a higher risk of harm than benefit should not be performed. Ethical medicine demands careful risk-benefit assessment (see risk above) to protect patient well-being and consideration for alternative treatment paths (see low carbohydrate diet above).
4th Pillar of Medical Ethics – Justice
Justice—the ethical imperative to distribute limited healthcare resources fairly—is especially relevant as the use of costly GLP-1 medications has surged for obesity even as their use for diabetes declines, creating stark disparities in access between higher- and lower-income patients. With U.S. prices far exceeding those abroad and Senate projections estimating up to $1 trillion in annual prescription spending (and $411 billion if broadly used for obesity [59]), programs like Medicare and Medicaid face unsustainable strain that threatens access for those most at risk. Ethically, clinicians must balance promoting these effective treatments against financial constraints by prioritizing patients who will gain the most “potential years of life lost” (PYLL) benefit—particularly younger, severely affected individuals—and focus on prevention of type 2 diabetes. As Emanuel argued in NEJM [60], and Dellgren and colleagues reiterated in The Lancet [61] and Annals of Internal Medicine [62], blanket coverage denials are unjust; instead, targeted coverage for those with the strongest claims aligns with both cost-effectiveness and justice until policy, supply, and pricing reforms ensure equitable access.
Conclusion: Balancing Risks, Benefits, and Costs
GLP-1 receptor agonists have ushered in a revolutionary era in obesity and type 2 diabetes care—offering dramatic weight loss, improved glycemic control, and meaningful reductions in cardiovascular and renal risk—but their extraordinary benefits are tempered by significant side effects, high discontinuation rates, lifelong dependency, and annual price tags exceeding $12,000/patient and $1 trillion in annual prescription spending that threaten both individual patients and the sustainability of our healthcare system. As lifestyle is frontline therapy, low carbohydrate and ketogenic eating strategies are underutilized therapeutic strategies shown to be safe, and induce profound weight loss, diabetes remission, MASLD reversal, and neurological protection while saving $5000 to >$10,000 in healthcare costs per patient. GLP1 administration must be anchored in the four pillars of medical ethics—that maximizes benefit, minimizes harm, and ensures equitable care for the most vulnerable.
Appendix:
Comprehensive Video from the author: Once and Future Use of GLP1 In the Framework of The Four Pillars Of Medical Ethics
Download slides in the note section. Video is unlisted https://www.youtube.com/watch?v=41Ptth0lEnU
References
- Liu L, Chen J, Wang L, Chen C, Chen L. Association between different GLP-1 receptor agonists and gastrointestinal adverse reactions: A real-world disproportionality study based on FDA adverse event reporting system database. Front Endocrinol (Lausanne). 2022 Dec 7;13:1043789. doi: 10.3389/fendo.2022.1043789. PMID: 36568085; PMCID: PMC9770009.
- Aldhaleei WA, Abegaz TM, Bhagavathula AS. Glucagon-like Peptide-1 Receptor Agonists Associated Gastrointestinal Adverse Events: A Cross-Sectional Analysis of the National Institutes of Health All of Us Cohort. Pharmaceuticals (Basel). 2024 Feb 2;17(2):199. doi: 10.3390/ph17020199. PMID: 38399414; PMCID: PMC10891568.
- Neeland IJ, Linge J, Birkenfeld AL. Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies. Diabetes Obes Metab. 2024 Sep;26 Suppl 4:16-27. doi: 10.1111/dom.15728. Epub 2024 Jun 27. PMID: 38937282.
- Guo H, Guo Q, Li Z, Wang Z. Association between different GLP-1 receptor agonists and acute pancreatitis: case series and real-world pharmacovigilance analysis. Front Pharmacol. 2024 Nov 13;15:1461398. doi: 10.3389/fphar.2024.1461398. PMID: 39605914; PMCID: PMC11600108.
- Alenzi KA, Alsuhaibani D, Batarfi B, Alshammari TM. Pancreatitis with use of new diabetic medications: a real-world data study using the post-marketing FDA adverse event reporting system (FAERS) database. Front Pharmacol. 2024 May 27;15:1364110. doi: 10.3389/fphar.2024.1364110. PMID: 38860168; PMCID: PMC11163090.
- Monami M, Nreu B, Scatena A, Cresci B, Andreozzi F, Sesti G, Mannucci E. Safety issues with glucagon-like peptide-1 receptor agonists (pancreatitis, pancreatic cancer and cholelithiasis): Data from randomized controlled trials. Diabetes Obes Metab. 2017 Sep;19(9):1233-1241. doi: 10.1111/dom.12926. Epub 2017 Jun 20. PMID: 28244632.
- Scheen AJ. Pharmacokinetics and clinical use of incretin-based therapies in patients with chronic kidney disease and type 2 diabetes. Clin Pharmacokinet. 2015 Jan;54(1):1-21. doi: 10.1007/s40262-014-0198-2. PMID: 25331711.
- Kaakeh Y, Kanjee S, Boone K, Sutton J. Liraglutide-induced acute kidney injury. Pharmacotherapy. 2012 Jan;32(1):e7-11. doi: 10.1002/PHAR.1014. PMID: 22392833.
- Bezin, J, Gouverneur, A, Penichon, M, et al. GLP-1 receptor agonists and the risk of thyroid Cancer. Diabetes Care. (2023) 46:384–90. doi: 10.2337/DC22-1148
- Das SR, Everett BM, Birtcher KK, Brown JM, Januzzi JL Jr, Kalyani RR, Kosiborod M, Magwire M, Morris PB, Neumiller JJ, Sperling LS. 2020 Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020 Sep 1;76(9):1117-1145. doi: 10.1016/j.jacc.2020.05.037. Epub 2020 Aug 5. PMID: 32771263; PMCID: PMC7545583.
- Prime Therapeutics. (2024). Real-world analysis of GLP-1a drugs for weight loss finds low adherence and increased cost in first year.. (https://www.primetherapeutics.com/news/real-world-analysis-of-glp-1a-drugs-for-weight-loss-finds-low-adherence-and-increased-cost-in-first-year/).
- Xie Y, Choi T, Al-Aly Z. Mapping the effectiveness and risks of GLP-1 receptor agonists. Nature Medicine. Jan. 20, 2025. DOI: https://doi.org/10.1038/s41591-024-03412-w
- Daniel J. Drucker ,The benefits of GLP-1 drugs beyond obesity. Science385,258-260(2024).DOI:10.1126/science.adn4128
- Ussher, J.R., Drucker, D.J. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol 20, 463–474 (2023). https://doi.org/10.1038/s41569-023-00849-3
- Kalyani RR. Glucose-Lowering Drugs to Reduce Cardiovascular Risk in Type 2 Diabetes. N Engl J Med. 2021 Apr 1;384(13):1248-1260. doi: 10.1056/NEJMcp2000280. PMID: 33789013.
- Uneda, K., Kawai, Y., Yamada, T. et al. Systematic review and meta-analysis for prevention of cardiovascular complications using GLP-1 receptor agonists and SGLT-2 inhibitors in obese diabetic patients. Sci Rep 11, 10166 (2021). https://doi.org/10.1038/s41598-021-89620-7
- Alexander JT, Staab EM, Wan W, Franco M, Knitter A, Skandari MR, Bolen S, Maruthur NM, Huang ES, Philipson LH, Winn AN, Thomas CC, Zeytinoglu M, Press VG, Tung EL, Gunter K, Bindon B, Jumani S, Laiteerapong N. The Longer-Term Benefits and Harms of Glucagon-Like Peptide-1 Receptor Agonists: a Systematic Review and Meta-Analysis. J Gen Intern Med. 2022 Feb;37(2):415-438. doi: 10.1007/s11606-021-07105-9. Epub 2021 Sep 10. PMID: 34508290; PMCID: PMC8810987.
- Christensen RM, Juhl CR, Torekov SS. Benefit-Risk Assessment of Obesity Drugs: Focus on Glucagon-like Peptide-1 Receptor Agonists. Drug Saf. 2019 Aug;42(8):957-971. doi: 10.1007/s40264-019-00812-7. Erratum in: Drug Saf. 2019 Jul;42(7):919. doi: 10.1007/s40264-019-00830-5. PMID: 30972641.
- De Barra C, Khalil M, Mat A, et al. Glucagon-like peptide-1 therapy in people with obesity restores natural killer cell metabolism and effector function. Obesity (Silver Spring). 2023; 31(7): 1787-1797. doi:10.1002/oby.23772
- Iorga RA, Bacalbasa N, Carsote M, Bratu OG, Stanescu AMA, Bungau S, Pantis C, Diaconu CC. Metabolic and cardiovascular benefits of GLP-1 agonists, besides the hypoglycemic effect (Review). Exp Ther Med. 2020 Sep;20(3):2396-2400. doi: 10.3892/etm.2020.8714. Epub 2020 May 5. PMID: 32765722; PMCID: PMC7401476.
- McCoy, R.G., Herrin, J., Swarna, K.S. et al. Effectiveness of glucose-lowering medications on cardiovascular outcomes in patients with type 2 diabetes at moderate cardiovascular risk. Nat Cardiovasc Res 3, 431–440 (2024). https://doi.org/10.1038/s44161-024-00453-9
- Bergmann NC, Davies MJ, Lingvay I, Knop FK. Semaglutide for the treatment of overweight and obesity: A review. Diabetes Obes Metab. 2023 Jan;25(1):18-35. doi: 10.1111/dom.14863. Epub 2022 Oct 18. PMID: 36254579; PMCID: PMC10092086.
- Wharton S, Batterham RL, Bhatta M, et al. Two-year effect of semaglutide 2.4 mg on control of eating in adults with overweight/obesity: STEP 5. Obesity (Silver Spring). 2023; 31(3): 703-715. doi:10.1002/oby.23673
- Ruseva, A, Michalak, W, Zhao, Z, Fabricatore, A, Hartaigh, B, and Umashanker, D. Semaglutide 2.4 mg clinical outcomes in patients with obesity or overweight in a real-world setting: a 6-month retrospective study in the United States (SCOPE). Obes Sci Pract. (2024) 10:e737. doi: 10.1002/OSP4.737
- Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes – state-of-the-art. Mol Metab. 2021 Apr;46:101102. doi: 10.1016/j.molmet.2020.101102. Epub 2020 Oct 14. PMID: 33068776; PMCID: PMC8085572.
- American Diabetes Association Professional Practice Committee; 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2025. Diabetes Care 1 January 2025; 48 (Supplement_1): S181–S206. https://doi.org/10.2337/dc25-S009
- Marsico F, Paolillo S, Gargiulo P, Bruzzese D, Dell’Aversana S, Esposito I, Renga F, Esposito L, Marciano C, Dellegrottaglie S, Iesu I, Perrone Filardi P. Effects of glucagon-like peptide-1 receptor agonists on major cardiovascular events in patients with Type 2 diabetes mellitus with or without established cardiovascular disease: a meta-analysis of randomized controlled trials. Eur Heart J. 2020 Sep 14;41(35):3346-3358. doi: 10.1093/eurheartj/ehaa082. PMID: 32077924.
- Madsbad S, Holst JJ. Cardiovascular effects of incretins: focus on glucagon-like peptide-1 receptor agonists. Cardiovasc Res. 2023 May 2;119(4):886-904. doi: 10.1093/cvr/cvac112. PMID: 35925683.
- Badve SV, Bilal A, Lee MMY, Sattar N, Gerstein HC, Ruff CT, McMurray JJV, Rossing P, Bakris G, Mahaffey KW, Mann JFE, Colhoun HM, Tuttle KR, Pratley RE, Perkovic V. Effects of GLP-1 receptor agonists on kidney and cardiovascular disease outcomes: a meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2025 Jan;13(1):15-28. doi: 10.1016/S2213-8587(24)00271-7. Epub 2024 Nov 25. PMID: 39608381.
- Chen JY, Hsu TW, Liu JH, Pan HC, Lai CF, Yang SY, Wu VC. Kidney and Cardiovascular Outcomes Among Patients With CKD Receiving GLP-1 Receptor Agonists: A Systematic Review and Meta-Analysis of Randomized Trials. Am J Kidney Dis. 2025 Jan 23:S0272-6386(25)00042-3. doi: 10.1053/j.ajkd.2024.11.013. Epub ahead of print. PMID: 39863261.
- Wang W, Wang QQ, Qi X, et al. Associations of semaglutide with first-time diagnosis of Alzheimer’s disease in patients with type 2 diabetes: Target trial emulation using nationwide real-world data in the US. Alzheimer’s Dement. 2024; 20: 8661–8672. https://doi.org/10.1002/alz.14313
- Kopp KO, Li Y, Glotfelty EJ, Tweedie D, Greig NH. Incretin-Based Multi-Agonist Peptides Are Neuroprotective and Anti-Inflammatory in Cellular Models of Neurodegeneration. Biomolecules. 2024 Jul 19;14(7):872. doi: 10.3390/biom14070872. PMID: 39062586; PMCID: PMC11275108.
- Hendershot CS, Bremmer MP, Paladino MB, et al. Once-Weekly Semaglutide in Adults With Alcohol Use Disorder: A Randomized Clinical Trial. JAMA Psychiatry. Published online February 12, 2025. doi:10.1001/jamapsychiatry.2024.4789
- Bruns Vi N, Tressler EH, Vendruscolo LF, Leggio L, Farokhnia M. IUPHAR review – Glucagon-like peptide-1 (GLP-1) and substance use disorders: An emerging pharmacotherapeutic target. Pharmacol Res. 2024 Sep;207:107312. doi: 10.1016/j.phrs.2024.107312. Epub 2024 Jul 18. PMID: 39032839; PMCID: PMC11467891.
- Farokhnia M, Tazare J, Pince CL, Bruns Vi N, Gray JC, Lo Re Iii V, Fiellin DA, Kranzler HR, Koob GF, Justice AC, Vendruscolo LF, Rentsch CT, Leggio L. Glucagon-like peptide-1 receptor agonists but not dipeptidyl peptidase-4 inhibitors reduce alcohol intake. J Clin Invest. 2025 Mar 6:e188314. doi: 10.1172/JCI188314. Epub ahead of print. PMID: 40048376.
- Patel Chavez C, Cusi K, Kadiyala S. The Emerging Role of Glucagon-like Peptide-1 Receptor Agonists for the Management of NAFLD. J Clin Endocrinol Metab. 2022 Jan 1;107(1):29-38. doi: 10.1210/clinem/dgab578. PMID: 34406410; PMCID: PMC8684453.
- Liao C, Liang X, Zhang X, Li Y. The effects of GLP-1 receptor agonists on visceral fat and liver ectopic fat in an adult population with or without diabetes and nonalcoholic fatty liver disease: A systematic review and meta-analysis. PLoS One. 2023 Aug 24;18(8):e0289616. doi: 10.1371/journal.pone.0289616. PMID: 37616255; PMCID: PMC10449217.
- Meurot C, Martin C, Sudre L, Breton J, Bougault C, Rattenbach R, Bismuth K, Jacques C, Berenbaum F. Liraglutide, a glucagon-like peptide 1 receptor agonist, exerts analgesic, anti-inflammatory and anti-degradative actions in osteoarthritis. Sci Rep. 2022 Jan 28;12(1):1567. doi: 10.1038/s41598-022-05323-7. PMID: 35091584; PMCID: PMC8799666.
- Ryan M, Megyeri S, Nuffer W, Trujillo JM. The potential role of GLP-1 receptor agonists in osteoarthritis. Pharmacotherapy. 2025 Mar;45(3):177-186. doi: 10.1002/phar.70005. Epub 2025 Feb 20. PMID: 39980227.
- Critical appraisal for low-carbohydrate diet in nonalcoholic fatty liver disease: Review and meta-analyses Ahn, Jaehee et al. Clinical Nutrition, Volume 38, Issue 5, 2023 – 2030
- Foster GD, Wyatt HR, Hill JO, McGuckin BG, Brill C, Mohammed BS, Szapary PO, Rader DJ, Edman JS, Klein S. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med. 2003 May 22;348(21):2082-90. doi: 10.1056/NEJMoa022207. PMID: 12761365.
- McKenzie AL, Athinarayanan SJ, Van Tieghem MR, Volk BM, Roberts CGP, Adams RN, Volek JS, Phinney SD, Hallberg SJ. 5-Year effects of a novel continuous remote care model with carbohydrate-restricted nutrition therapy including nutritional ketosis in type 2 diabetes: An extension study. Diabetes Res Clin Pract. 2024 Nov;217:111898. doi: 10.1016/j.diabres.2024.111898. Epub 2024 Oct 20. PMID: 39433217.
- Athinarayanan SJ, Adams RN, Hallberg SJ, McKenzie AL, Bhanpuri NH, Campbell WW, Volek JS, Phinney SD, McCarter JP. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-randomized Clinical Trial. Front Endocrinol (Lausanne). 2019 Jun 5;10:348. doi: 10.3389/fendo.2019.00348. PMID: 31231311; PMCID: PMC6561315.
- Goldenberg JZ, Day A, Brinkworth GD, Sato J, Yamada S, Jönsson T, Beardsley J, Johnson JA, Thabane L, Johnston BC. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: systematic review and meta-analysis of published and unpublished randomized trial data. BMJ. 2021 Jan 13;372:m4743. doi: 10.1136/bmj.m4743. PMID: 33441384; PMCID: PMC7804828.
- Critical appraisal for low-carbohydrate diet in nonalcoholic fatty liver disease: Review and meta-analyses Ahn, Jaehee et al. Clinical Nutrition, Volume 38, Issue 5, 2023 – 2030
- Childhood Obesity Vol. 9, No. 3 A Low-Glycemic-Load versus Low-Fat Diet in the Treatment of Fatty Liver in Obese Children, https://doi.org/10.1089/chi.2013.0022
- https://www.virtahealth.com/press/virta-healths-diabetes-reversal-treatment-drives-savings-of-more-than-10k-per-patient-over-two-years-new-analysis-shows
- Buchanan L, Calkins M, Kalayjian T, Norwitz NG, Teicholz N, Unwin D, Soto-Mota A. TOWARD, a metabolic health intervention, demonstrates robust 1-year weight loss and cost-savings through deprescription. Front Nutr. 2025 Feb 14;12:1548609. doi: 10.3389/fnut.2025.1548609. PMID: 40028226; PMCID: PMC11868080.
- Watso JC, Robinson AT, Singar SAB, Cuba JN, Koutnik AP. Advanced cardiovascular physiology in an individual with type 1 diabetes after 10-year ketogenic diet. Am J Physiol Cell Physiol. 2024 Aug 1;327(2):C446-C461. doi: 10.1152/ajpcell.00694.2023. Epub 2024 Jun 24. PMID: 38912731; PMCID: PMC11427101.
- ANDREW P. KOUTNIK, THOMAS WOOD, KRISTI STOROSCHUK, BELINDA S. LENNERZ; 608-P: Carbohydrate Intake, Glycemic Control, and Cardiometabolic Risk Factors in Type 1 Diabetes—A Systematic Review and Meta-regression. Diabetes 14 June 2024; 73 (Supplement_1): 608–P. https://doi.org/10.2337/db24-608-P
- J Clin Invest. 2021;131(1):e142246. https://doi.org/10.1172/JCI142246.
- Front. Nutr. , 08 February 2023 Volume 10 – 2023 | https://doi.org/10.3389/fnut.2023.1084021
- Dorans KS, Bazzano LA, Qi L, et al. Effects of a Low-Carbohydrate Dietary Intervention on Hemoglobin A1c: A Randomized Clinical Trial. JAMA Netw Open. 2022;5(10):e2238645. doi:10.1001/jamanetworkopen.2022.38645
- Devi N, Madaan P, Kandoth N, Bansal D, Sahu JK. Efficacy and Safety of Dietary Therapies for Childhood Drug-Resistant Epilepsy: A Systematic Review and Network Meta-analysis. JAMA Pediatr. 2023;177(3):258–266. doi:10.1001/jamapediatrics.2022.5648
- Martinez, C.C., Pyzik, P.L. and Kossoff, E.H. (2007), Discontinuing the Ketogenic Diet in Seizure-Free Children: Recurrence and Risk Factors. Epilepsia, 48: 187-190. https://doi.org/10.1111/j.1528-1167.2006.00911.x
- Liyang Rong, Yating Peng, Qi Shen, Keying Chen, Bangjiang Fang, Weirong Li, Effects of ketogenic diet on cognitive function of patients with Alzheimer’s disease: a systematic review and meta-analysis,The Journal of nutrition, health and aging,Volume 28, Issue 8,2024,100306, ISSN 1279-7707, https://doi.org/10.1016/j.jnha.2024.100306.
- Fortier M, Castellano C-A, St-Pierre V, et al. A ketogenic drink improves cognition in mild cognitive impairment: Results of a 6-month RCT. Alzheimer’s Dement. 2021; 17: 543–552. https://doi.org/10.1002/alz.12206
- Oehm S, Steinke K, Schmidt J, Arjune S, Todorova P, Heinrich Lindemann C, Wöstmann F, Meyer F, Siedek F, Weimbs T, Müller RU, Grundmann F. RESET-PKD: a pilot trial on short-term ketogenic interventions in autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 2023 Jun 30;38(7):1623-1635. doi: 10.1093/ndt/gfac311. PMID: 36423335; PMCID: PMC10435930.
- https://www.help.senate.gov/dem/newsroom/press/news-chairman-sanders-releases-report-exposing-how-weight-loss-drugs-could-bankrupt-american-health-care
- Emanuel EJ, Dellgren JL, McCoy MS, Persad G. Fair Allocation of GLP-1 and Dual GLP-1-GIP Receptor Agonists. N Engl J Med. 2024 May 30;390(20):1839-1842. doi: 10.1056/NEJMp2400978. Epub 2024 Apr 17. PMID: 38630999
- International coverage of GLP-1 receptor agonists: a review and ethical analysis of discordant approaches; Dellgren, Johan L et al. The Lancet, Volume 404, Issue 10455, 902 – 906
- Dellgren J, Emanuel E, Persad G. Ethical Approaches to Limiting Overall Costs for Glucagon-Like Peptide-1 Receptor Agonists for Weight Management. Ann Intern Med. 2025 Jan;178(1):119-121. doi: 10.7326/ANNALS-24-01317. Epub 2024 Nov 26. PMID: 39586102.